

TB patient hospitalized in Svay Rieng Provincial Hospital, Cambodia.Photo by James Nachtwey
Healing TB in Cambodia and the world
Tuberculosis is curable—whether in the world’s wealthiest countries or in its poorest. But in 1994 when Cambodian Health Committee was founded, the access to TB treatment and care in Cambodia was nearly nonexistent, a country, which had been ravaged by 2 decades of war, and where extreme poverty was widespread.
With a collapsed health system and poor access to care in a country of farmers at the time, Cambodia had become a global TB hotspot with one of the highest rates of TB in the world.
And at the time, it was widely believed by international agencies that poor, rural communities were incapable of completing the lengthy 6–8 month TB treatment that was necessary for cure.
Cambodian Health Committee (CHC) changed that. Starting from the ground up, CHC built a community-based TB program working in coordination with the National TB Program that overcame every barrier—delivering care through local health workers, bringing treatment to patients' homes, and proving that even the poorest could be cured with the right programatic support.
CHC’s work is grounded in the belief that access to treatment for a curable disease like TB is a human right—and that with the right support, anyone, anywhere, can complete the long and difficult treatment.
Our Origins: From Refugee Camp to Lifesaving Care in Cambodia
CHC’s roots trace back to the refugee camps on the Thai-Cambodian border, where survivors of the Khmer Rouge genocide fled in the 1980s. It was there in 1981 that Steve Miles and Bob Maat working with the American Refugee Committee (ARC) started a groundbreaking TB program -- whose radical approach introduced TB treatment contracts, TB education, food assistance, and patient supporters to TB care and showed that refugees could be treated for this fatal yet, curable disease as they reported. These data defied global expert opinions that argued that refugees with TB couldn’t be treated in a war zone—that they would not complete the 6 month treatment. As Steve Miles wrote at the time, and which is true today, “TB is…about a debilitating, lethal, contagious and curable illness”.
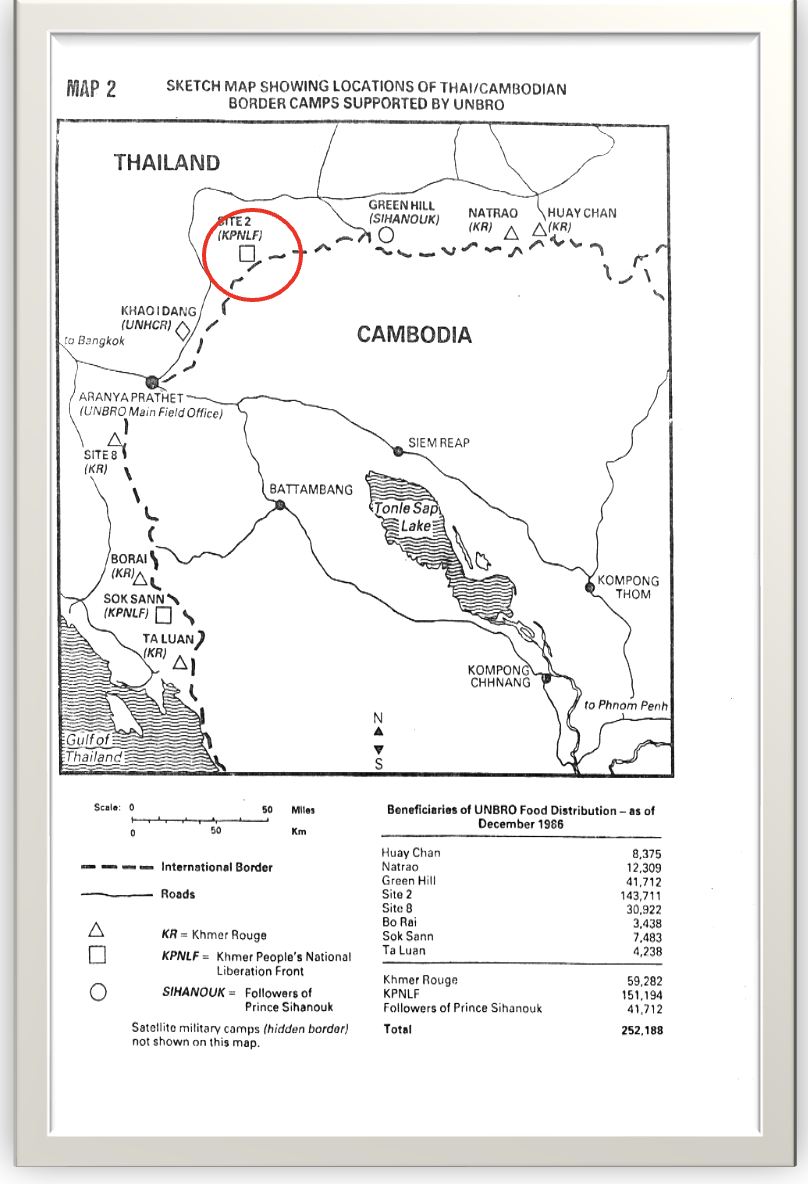
In 1989, co-founders of Cambodian Health Committee, Sok Thim, Anne Goldfeld, and Brian Heidel, met while working with the American Refugee Committee (ARC) at the Site II refugee camp on the Thai-Cambodian border (Site II is circled on the map below). Sok Thim, who graduated from ARC’s medic training program, was trained by Bob Maat and took over coordination of the TB Program at Site II. He was then secunded to the UN Border Relief Organization (UNBRO) where he supervised TB programs in all the refugee camps on the border camps (graphic below). The ARC program would treat over 3000 patients in the border camps before the refugees returned to Cambodia.
In the early 1990s when the refugees returned to Cambodia, they found a country devastated by decades of war, which had no functioning health care system or effective TB treatment program. Even among those citizens who accessed TB treatment, only ~20% completed the required 6-month regimen for cure leaving them still sick, contagious, and susceptible to developing drug resistant TB.
In response, the WHO and French Red Cross advised Cambodia to require forced hospitalization for the first 2 months of TB treatment—a policy that was impossible for poor farming families, who couldn’t afford to leave their fields. Even after hospitalization, the long distances and cost of monthly medication pick-up meant patients often dropped out of treatment before completing the 6 month long treatment. Many never sought treatment until it was too late.
In 1994, with seed support from the Blue Oak and Christopher Reynolds Foundations, the Cambodian Health Committee (CHC) was launched and chose to work in Svay Rieng, one of Cambodia’s poorest provinces with the highest rate of TB infection in the country, to bring TB treatment to the people who needed it the most.
Building on the lessons learned in the life-saving refugee-camp program, CHC brought the transformative TB approaches of patient supporters, food supplementation, education about TB disease, treatment contracts, and observed consumption of TB medications to rural Cambodia in 1994, where at the time a family of 7 lived on less than $220/year and TB prevalence was among the highest in the world estimated to be ~900 individuals with TB/per 100,000 citizens.
CHC developed a new model in Cambodia working with the National TB Program: community-based TB care rooted in dignity, support, and science. CHC’s work became a national health intervention—transforming TB care across Cambodia and went on to influence programs across the world from Haiti to Ethiopia to Vietnam.
Bringing TB Care to post-conflict Cambodia
Meeting the situation in impoverished rural Cambodia, CHC developed and added new solutions to bring TB care to the community and to patient homes, including:
Food as Complementary Medicine: Pioneered with the World Food Program, CHC delivered monthly food packages with medicine pickups—now a global best practice.
Expanding the Role of Patient Supporters: Supporters, patients, and medical staff signed a treatment contract committing each partner to work together to achieve a cure. Patient supporters were trained to monitor daily therapy of TB medicine at home and accompany the patients through therapy.
Establishing Mobile TB Teams: CHC launched mobile health worker teams who visited patients at home, to check how the patients were managing to take their medications, while screening other family members for TB infection. If there was an interruption of therapy, the team strategizes with the patient and the supporter about any issues interfering with their TB treatment and how to overcome them.
Active TB case finding in villages: Mobile CHC teams screened clusters of villages -- going house-to-house -- to find people who may be suffering from TB, rather than waiting for them to seek help at the health center. In this way, TB was be diagnosed and treated earlier, before the infection had caused irreversible impact on patients’ lungs and health.
TB HOME CARE by CHC mobile teams and patient supporters: This pilot approach involved mobile TB health teams visiting each patient in their home 5 days a week during the initial two-month intensive phase of TB therapy to observe the patient taking their TB medication with the patient supporter supervising the treatment on the weekends. Among 219 TB HOME CARE patients, 100% of patients took their mediation daily and their cure rate was 99%.
Linking Poverty Reduction: Village banks focused on TB patients and families afflicted by TB, offered low interest loans based on the Grameen Bank model. And for example, among 590 TB patients who joined the village bank program between 1995 to 2000, TB treatment adherence and cure were each 100%, and loan payback was 100%. In the same period, a Village Health Fund was created from interest on loan payback that trained Village Health Agents in 96 villages, who performed TB case finding and spread TB health messages.
The results of the CHC Program described above were published in the Journal of the American Medical Association in 2004.
These community innovations put CHC in a position to transform Cambodia’s TB response in partnership with the National TB Program and led to the development with the Cambodian National TB Program of community TB care or Community Daily Observed Therapy (or c-DOTS), which changed the trajectory of the TB disaster in Cambodia to one of great success in TB treatment globally in the early 2000s.
Bringing TB care to those who live far from health centers: CHC’s Community TB Care
Community Treatment or Community DOTS, as it came to be known, was piloted by CHC in partnership with the National TB Program in Svay Rieng and Kompot Provinces with support from JICA (Japanese International Cooperation Agency). In 2006 it achieved a 95% TB cure rate—a game-changing success leading to its national scale-up.
The Community TB Treatment model trained local volunteers—including former TB patients—to serve as treatment supporters, helping neighbors stick to their daily medications by Daily Observed Treatment (DOTS) of the patient taking their TB medication.
CHC’s mobile teams guide both local Health Center staff, patients and supporters (called DOT watchers), through each phase of treatment, and through community trainings resulting in enhanced detection, education, and cure.
The CHC pilot worked so well, it was adopted for nationwide scale-up in Cambodia by the National TB Program with support from the Global Fund for TB, Malaria, and AIDS.
The World Health Organization (WHO) credited CHC’s Community ‘DOTS’ TB model—that was developed by CHC in Svay Rieng, piloted by CHC in Svay Rieng and Kompot provinces between 2003-2006, and subsequently scaled up throughout the country with the National TB Program—for the dramatic reduction of TB in Cambodia, citing it as a global model of success.
CHC’s Impact: 1994–2025
From 1994 to 2024, CHC has provided community-based TB care to over 110,000 Cambodians in partnership with the Cambodian National TB Program (NTP)—with adherence and cure rates in most years approaching or surpassing 95%.
In 2024, CHC treated 11,361 people with TB across 13 provinces in Cambodia covering a catchment area of nearly 7 million people, achieving a 97% cure rate.
CHC initiated the countrywide program for drug resistant (DR)-TB in Cambodia in 2006 and scaled it up throughout Cambodia with the National TB program, transferring its management to the NTP in 2012. 2100 patients have been initiated on DR-TB treatment from 2006-2025. To learn more about CHC’s work in DR-RB, please click here.
CHC pioneered provision of food with TB care in partnership with the World Food Program, which is now done globally
CHC introduced innovative strategies into TB care—including the idea of patient supporters, treatment contracts, food supplementation, poverty mitigation, home visits, and patient travel support to pick up medicines—strategies which improved case detection, adherence, and cure rates, which have been widely emulated globally.
CHC pioneered linking microfinance strategies with TB care.
CHC scaled up Community TB Care in Cambodia (called TB Community DOTS or cDOTS) with the National TB Program throughout Cambodia, and have played a critical role in reducing TB incidence nationwide, transforming Cambodia from one of the most TB-plagued countries in the world, to a global model of success in TB treatment and TB reduction.



In rural areas patients often live far from the Health Center or Hospital. The CHC team on their way to visit a TB patient in Svay Rieng for a follow-up visit.


HOME TB-CARE and active case-finding. This young father of two (upper left) is a farmer who had symptoms of lung TB for 2 months when he was found to have TB as the CHC team screened villagers house-by house. There was a significantly shorter delay between onset of symptoms and diagnosis of TB in patients who were found in the Home Care active house-to-house screening compared to patient who went to the health center with their symptoms. Patients often ignored their symptoms before going to figure what the problem was, was on average after 30 months or 2.5 years of symptoms. Patient found by house-to-house screening had symptoms for an average of only 6 months. The patient here, had been coughing for 6 months when the CHC TB-HOME Care Team found him and diagnosed TB. He achieved TB cure after 6 months of treatment with no long term complications to his lungs, likely because his TB was discovered so soon after his symptoms began by active screening for new TB disease. The right photo shows the TB team screening the patient’s children and his wife for TB, which is another advantage of TB Home Care, as family members could be promptly treated if they had evidence of TB.


This young woman and her husband (photo above left) are rice farmers in eastern Svay Rieng near the border of Vietnam. She was found to have TB during house-to-house screening for TB, luckily when the disease was caught early. She was cured of TB, with no lingering problems and gave birth to a son (upper photo left). A participant in the TB-linked village bank program, she used her capital to help buy a female water buffalo (photo on the right), which she rented out for farming, who gave birth to a baby buffalo (seen in the background of the photo), improving the economy and assets of the family.
TB patients waiting to be evaluated for TB outside the Kampong Ro Hospital in Svay Rieng, Cambodia 1995.
Healing the world one life at a time
CHC TB team visiting a farmer at home who had begun TB treatment to check on his progress on treatment. Svay Rieng 1997.